

Background
Due to intrinsic biological and treatment related factors, patients with multiple myeloma (MM) are at increased risk of hematologic second primary malignancies (SPMs). The risk of secondary myeloid neoplasms including myelodysplastic syndrome and acute myeloid leukemia (s-AML) have been well described in both MGUS and MM patients, particularly after melphalan and lenalidomide therapy. While the risk and outcomes of s-AML have been well-described, data on secondary acute lymphoblastic leukemia (s-ALL) are scant, and largely limited to case reports. The causative factor of s-ALL is felt to be related to lenalidomide use, which can increase mutational burden in immunoglobulin superfamily-3 (IGSF3) and CXXC4 (Wnt signaling pathway), although the large overall survival benefit outweighs this risk. To our knowledge, this is the first population-based study assessing s-ALL in MM patients. We aim to better characterize the demographic and survival outcome data of this rare entity and make comparisons to the better studied s-AML.
Methods
The Surveillance, Epidemiology, and End Results (SEER)-18 database was utilized which covers 35% of the U.S. population. Inclusion criteria was as follows: 1) 18 years of age or older at time of diagnosis, 2) diagnosed with MM, 3) diagnosed with s-ALL and s-AML by selected ICD-O codes and 4) MM and s-ALL/s-AML diagnoses occurred between 2000-2016. Analyses were conducted with STATA Version 14.2 (College Station, TX). Data were censored at time of death or loss to follow up. Kaplan-Meier curves were generated to demonstrate overall survival (OS).
Results
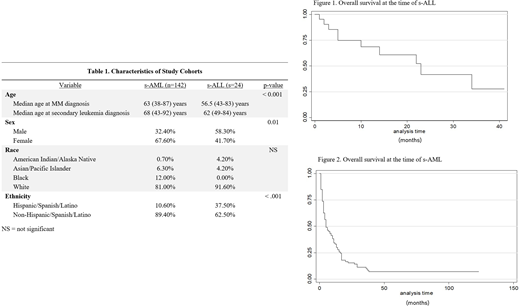
Among 86,405 adult MM subjects identified in SEER from 2000-2016, 166 met inclusion criteria for secondary leukemias. Of these, 24 were s-ALL with an overall incidence of 0.03%. Among s-ALL subjects in this study, B-ALL was the most frequent histology (66.7%), followed by precursor B-ALL (12.5%) and Burkitt's leukemia (8.3%). Median age at secondary leukemia diagnosis was lower at 62 (49-84) years for s-ALL compared to 68 years for s-AML (43-92) (p< 0.001). Other significant differences in patient characteristics include s-ALL subjects more commonly being male (58.3% versus 32.4%, p=0.01) and Hispanic (37.5% versus 10.6%, p<0.001). Leukemia was the most frequent cause of death in both s-ALL and s-AML. Median OS was 23 months in s-ALL compared to 5 months in s-AML.
Discussion
In our analysis, secondary ALL occurred in less than 1 of every 3,000 MM patients. While there were six times more s-AML cases than s-ALL, those with s-ALL lived nearly five times longer than s-AML patients. This aligns with primary ALL data in adults who have greater than twice the 5-year survival of primary AML after adjusting for age. There were also significant differences by age, gender and ethnicity when compared to the more common s-AML, raising the question of what other genetic and environmental factors may influence the development of s-ALL. Although lenalidomide has been thought to be the culprit of s-ALL, the overall survival benefit far outweighs this rare risk. Given its rarity, further studies are needed to better understand the pathogenesis and treatment outcomes of s-ALL in MM patients.
Disclosure
The findings and opinions contained herein are those of the authors and do not represent the views/opinions of the United States Air Force, Walter Reed National Military Medical Center, David Grant Medical Center, or the Department of Defense.
No relevant conflicts of interest to declare.

